


A Brief Anecdote Re: Involuntary Psychiatric Treatment
A case of catatonia

As always, details and identifying information have been altered to preserve patient anonymity.
Case: “Uzma” is a 50 year old Pakistani woman with a known history of schizophrenia who was psychiatrically admitted due to worsening psychosis, inability to care for herself, and her family’s inability to manage her declining state. She has not been taking any medication for an unspecified period of time, likely months.
Before seeing her, nursing informed me she had refused all medications since arriving last night. I walked into her room with the case therapist. Uzma was sitting almost completely motionless on a chair by her desk, facing the window. She did not respond to her name. We walked over and observed her staring out the window, muttering repetitively, incomprehensibly, and almost inaudibly to herself. She rarely blinked. She only acknowledged us slowly when I waved my hand in front of her face. She could nod slightly when I said her name. When I asked her why she thought she was admitted she said after a long pause, “I’m pregnant” (she was not, of course). I asked if I could shake her hand and she shook her head no, saying, “I am a Muslimah, I am married.” (She had been divorced for many years). She continued to trail on like a broken record, repeating “Muslimah, Muslimah, Muslimah…” for almost a minute before stopping and staring out the window again.
“Ok, Uzma,” I said, “But, I do need to examine you, though. I’m just going to hold your left arm in my hands and move it around a bit. Won’t hurt at all. Just make your arm limp like it’s a wet noodle and let me move it for you.”
She did not respond or resist. I took her arm in my hands, flexing and extending her wrist, elbow, and shoulder joints through their normal ranges of motion. She was rigid, moreso at the outset of movement and then gradually easing. When I released her arm over her head, it remained fixed in place for a number of seconds before slowly descending down again. I repeated with her right arm with identical results, moving it across her chest as if to rest it on her left shoulder, but releasing it mid air, where it remained suspended before eventually falling slowly.
Her immobility, verbigeration alternating with mutism, staring, rigidity, and waxy flexibility with maintenance of unusual body postures were all signs of catatonia.1 Catatonia is a commonly occurring yet poorly understood syndrome, usually presenting as a hypoactive or “retarded catatonia” but in a minority of cases as a hyperactive condition, “excited catatonia”. It can also be mixed, alternating hyper- and hypoactivity. Catatonia is not an illness itself, but rather a syndrome that can result from any number of underlying CNS conditions such as bipolar disorder, major depression, schizophrenia, autism, drugs/substances, autoimmune encephalitis, cancer, epilepsy, and so on.
The prolonged immobility in catatonia can lead to deep vein thrombosis (DVT) and pulmonary embolism (PE), pressure ulcers, malnutrition, and muscle breakdown leading to rhabdomyolysis and kidney failure, among other complications. Those with excited catatonia can injury themselves or others unwittingly. The rigidity can be so bad that some people display the “pillow sign” in which the patient appears to by lying on her back in bed, but on closer examination the head, neck, and sometimes back are slightly raised off the bed and remain suspended sometimes for hours or more. To try this yourself, lie down on your back with your hands at your side. Then start to raise your upper body up using your core, as if you’re about to sit upright. When your head, neck, and back are about an inch off the bed, stop moving and maintain that position for as long as you can.
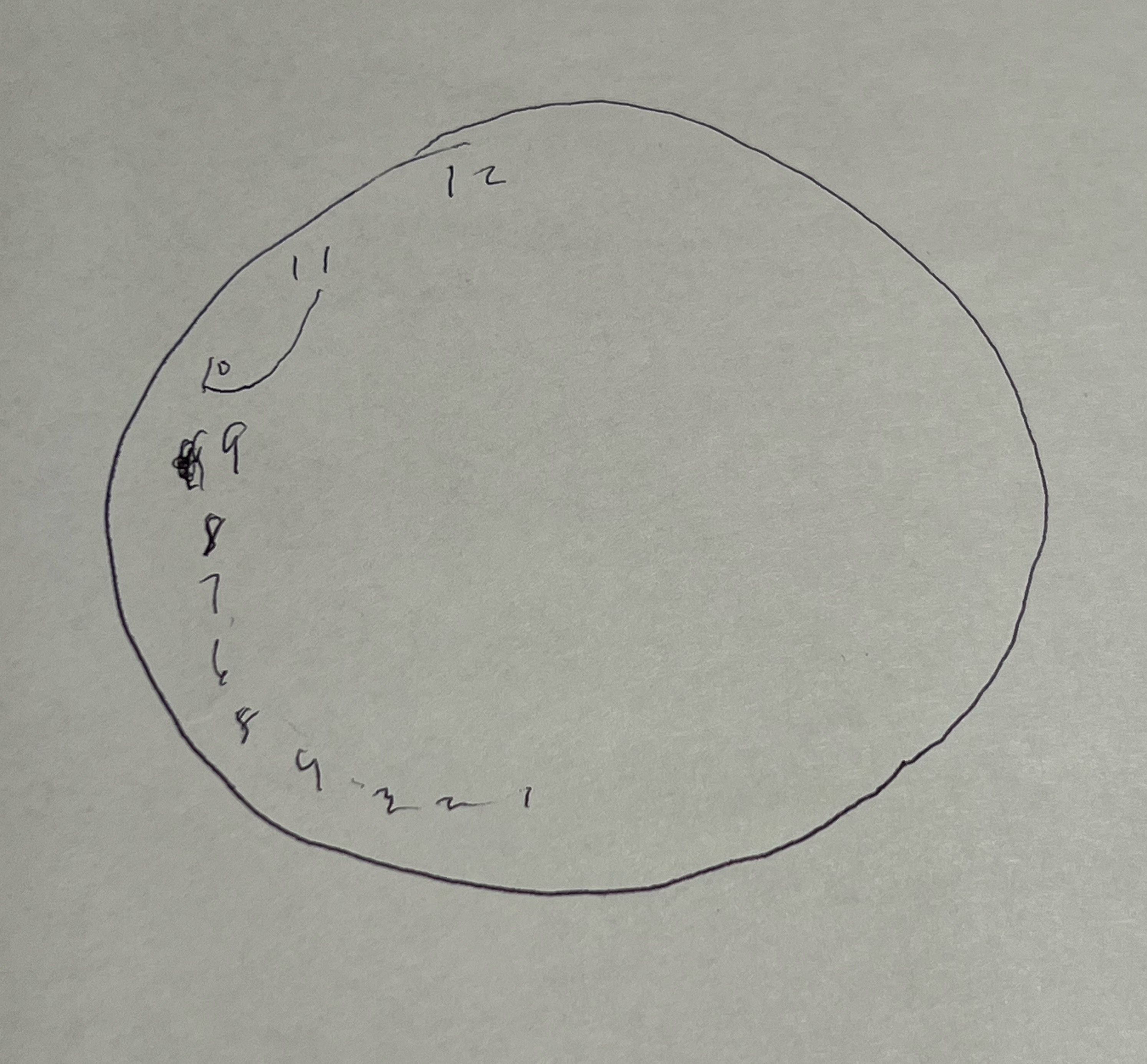
If you’ve read my earlier post (link below), then you’ll remember that catatonic people draw very weird and interesting clocks.

I asked Uzma to draw a clock with the time set to 11:10. I had to place the pen in her hand, wrap her fingers around it, and place the paper in front of her. She produced the drawing below, starting with a good circle, then placing the 12, and working backwards. Her pace slowed as she went, the numbers get closer together and around number 6 she totally loses the thread. She makes an attempt to connect the 11 to the 10, then places the pen down and goes back to staring out the window. Her movements were slowed such that it took around 3 or 4 minutes to complete the clock.
“Uzma, we’re going to get some medicine to help you,” I said.
“No medicine,” she mumbled, shaking her head. We went back and forth a while. I got the feeling she didn’t want the voices she was hallucinating to go away, and knew that medication might make that happen.
“Uzma, we have to give you something to help your muscles relax. This won’t make the voices go away. But you aren’t eating or drinking and this will help you move around and drink water.”
Eventually she agreed and took lorazepam (brand name Ativan). Benzodiazepines—lorazepam in particular—are both a diagnostic test to confirm catatonia, as well as a first line treatment (the definitive treatment is electroconvulsive therapy). If catatonia is suspected, give 2 mg lorazepam IV or IM, and within minutes to around an hour most patients start “waking up” and regaining some normal function. This response confirms the diagnosis. You then either continue treating with benzodiazepines, or moves on to electroconvulsive therapy, depending on the circumstances.2
Within 20 minutes or so, Uzma was up and out of her chair, able to walk and drink water. Later, she adamantly refused another dose of lorazepam, however, and started becoming catatonic again by the late afternoon. We filed the necessary paperwork for court-mandated treatment given her inability to voluntarily consent to treatment and her utterly non-functional condition. It would probably take about a week for the county to get the hearing set up and a ruling issued.
The next morning I saw her she was again sitting at her chair, still hypokinetic and staring out the window. The only word she would say is “praying”, which was perhaps what the mumbling was. She was now drooling as well, a puddle slowly forming in her lap. She did not seem to notice or make efforts to wipe it away. Her physical exam was unchanged from yesterday, all catatonic signs still present. She refused lorazepam and I couldn’t convince her otherwise.
Her vitals were stable. This is important because, aside from DVTs and the other sequelae I listed above, catatonia can also progress into something called malignant catatonia, where your autonomic nervous system starts going haywire in very scary ways and is often fatal if untreated. She was stable for now, but I had no way of knowing that she would remain so for the week until the court hearing. What happens if she refuses lorazepam for a few days and progresses to malignant catatonia in the middle of the night? In this case I knew she needed some lorazepam to get her through the week, otherwise things could get dicey.
The case therapist and I called the hospital’s Risk Department to make sure everyone was on the same page, since there are some pretty strict rules regarding giving psychiatric medication against someone’s will. We talked the case over and explained the need to give lorazepam involuntarily despite not having a court order yet. They readily agreed that administering the medication against the patient’s will was clearly in her best interest and was justified. Given her precarious condition and risk of major morbidity or mortality, there was obviously no excuse not to act in some way.
We arranged to have lorazepam administered involuntarily until the court hearing, which would help keep her medically stable until more definitive treatment could be approved.
I’m writing this up both because it’s an interesting case, but also because those who critique the practice of involuntary treatment tend not to use examples like this to make their point. And cases like this are very common!
See the Bush-Francis catatonia rating scale (BFCRS) for a brief description of catatonic signs.
https://thompsoncenter.missouri.edu/wp-content/uploads/2019/04/Bush-Francis-Scale-with-a-few-references-4-18-19.pdf
Sometimes you need very high dose benzodiazepines. In one particularly severe case of excited catatonia where electroconvulsive therapy was not available, a patient was being given up to 26 mg lorazepam IV daily and was still practically doing backflips off the hospital bed (26 mg of Ativan is a lot).
In addition to the physical risks you mention, the subjective experience of catatonia is often terrible beyond description. Delusions may impel someone to believe it is also important or meaningful to exist in that state, but relief from catatonia is rescue from an extremis of psychological torture most are fortunate to never experience. Despite being the most salient aspect of catatonia for those who experience it, I find this is rarely mentioned. Another compelling reason to act quickly to provide relief, even over the objections of the patient.
If I or another family member ever suffer from catatonia, I sure hope our doctor is as caring and knowledgeable as Dr. Greenwald. It pains me to see our streets riddled with individuals suffering from severe mental illness without any treatment. In my opinion, their "freedom" does not add to their quality of life.